Last Updated on October 22, 2022
“Knowing how to insert branula is not enough. A doctor should also master chest tube insertion, as good as branula insertion”
Introduction
2 methods
• Open method
• Closed method (do not use this method)
Important parts of a chest tube
• Radio-opaque tip and a marker strip along the edge
• Fenestrated end (with holes for drainage of air / fluid)
Chest drainage system
Types
• Single-bottle system (underwater seal)
• Two-compartment system (underwater seal)
• Three-compartment system (underwater seal)
• Wet-suction
• Dry suction
Underwater seal system – 1-bottle system
• Tip of the rigid straw is immersed at least 2 cm below surface of water
• Disadvantages
=====
Further reading:
Chest drainage systems in use, by NIH
Underwater seal drainage system, by LITFL
Inspiration, by LibreTexts
Chest tube Insertion
Indications
(i) Pneumothorax / tension pneumothorax
(ii) Pleural effusion
• Empyema
• Haemothorax
• Chylothorax
(iii) Post-op
• Post thoracotomy
• Post VATS
Complications
During insertion
• Injury to internal organs / structures e.g. heart, liver, spleen, diaphragm
• Bleeding
Post-insertion
• Infection
• Subcutaneous emphysema
• Improper placement / Chest tube dislodgement
• Re-expansion pulmonary oedema
Equipment
• Gown, sterile gloves, mask
• Sterile drapes
• Dressing set / ‘Pneumothorax set’
• Gauze
• Antiseptic solution e.g. chlorhexidine
• Curved blunt artery forceps
• Needle holder
• Scissors
• Scalpel blade size 10
• Syringe: 10 mL x2
• Needle: 1 green, 1 blue needle
• Adhesive dressing tape (e.g. Hypafix®)
• Lignocaine 1%
• Suture — Silk O
• Chest tube of appropriate size
Pre-Insertion
• Ensure correct indications
• Ensure correct patient
• Ensure correct site
• Consent
Inserting a chest tube
• Mark the safety triangle
• Positioning
• Clean area of insertion with antiseptic solution
• Drape the area of insertion
• Syringe out 1% lignocaine then infiltrate to the area of interest (using blue needle)
• Use scalpel bladeto make a 2 – 4 cm skin incision near upper border of the rib below (at 5th intercostal space), and just anterior to mid-axillary line
• Once subcutaneous layer is cut, split muscle layers using curved blunt artery forceps till the level of pleura
• Use curved blunt artery forceps to pass through the parietal pleura
• Insert your index finger to widen the tract, then feel for the lung and check for adhesion
• Remove trocar from the chest tube
• Place blunt artery forceps at the fenestrated end of chest tube
• Use blunt artery forceps to guide chest tube into pleural cavity, to the correct direction
• Release the blunt artery forceps, then advance the chest tube into pleural space
• Ensure all fenestrated areas are inside the pleural cavity
• Connect chest tube to underwater seal system
• Check whether the chest drain is functioning
• Secure chest tube with Silk 0 suture
• Also, suture the skin incision site
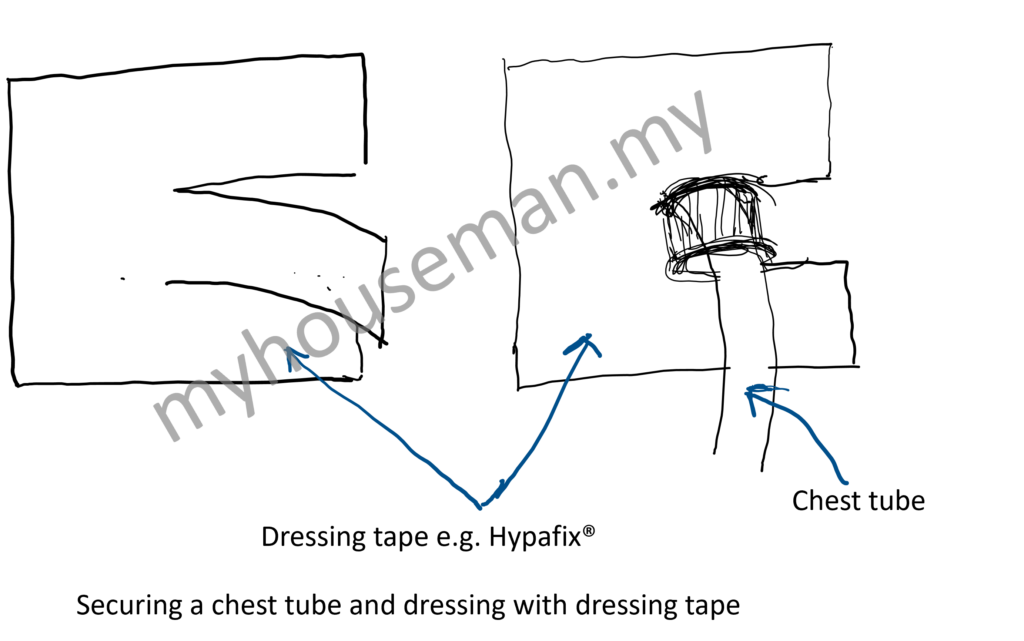
• Apply sterile occlusive dressing to the chest tube as shown below:
Video
Chest tube removal / Re-anchoring
Steps
• Teach patient Valsalva manoeuvre (i.e. breath holding on maximal inspiration
• Positioning of patient
• Prepare the equipment
• Clean the area of chest tube insertion site with chlorhexidine
• Drape the area of chest tube insertion site
• Clamp the chest tube e.g. using sponge forceps
• Make a pursed-string suture prior to removal of chest tube
• Instruct your assistant to pull out the chest tube when patient has inspired and is holding his breath
• Close the pursed-string suture simultaneously when your assistant is removing the chest tube, rapidly
Post chest tube removal
• Vital signs
• Examine the lungs: air entry bilaterally
• Repeat chest X ray
Chest tube removal / Re-anchoring set
• Dressing set
• Needle holder
• Stitch scissors
• Silk 0 suture (prepare 2)
• Gauze (prepare 2)
• Chlorhexidine
• 10 cc syringe
• Green needle; Blue needle
• Lignocaine for injection
• Tegaderm + dry gauze
Is the Chest Tube Functioning?
Yes, if:
• Periodic presence of air bubble in the underwater seal
• Fluctuation of fluid level in water-seal chamber / inside the chest tube
Other Knowledge Required
• Anatomy of safety triangle
• Suture technique e.g. Surgical Knot Tying: One-handed, pursed-string suture
Miscellaneous
• Do not insert chest tube into an open wound due to trauma. Instead, chest tube should be inserted at the ipsilateral side, as long as it’s inserted at safety triangle
Related Posts
Q&A
This content is restricted to subscribers